Hyperbaric Oxygen Treatment & MS
Background:Magnetic resonance spectroscopyhas shown that lactate, the hallmark of hypoxia (low tissue oxygen) is present in acute lesions. Blood–brain barrier disturbance precedes the symptoms and is involved in migration of auto-reactive T-cells into the nervous system. Hyperbaric oxygen has been shown to improve BBB integrity. Naturally, the oxygen rich environment is favorable for Myelin repair especially when appropriate building blocks are given such as Vitamin K, B12, Phospholipids/Citicholine, Methyl-Folate, Pregenolone and Essential fatty acids. Hyperbaric treatment allows for resumption of normal aerobic metabolism in acute areas affected by the disease process.
Hyperbaric Oxygen therapy ameliorated symptoms in Experimental Allergic Encephalomyelitis (EAE) the animal model of multiple sclerosis in numerous studies. Human Data:In 1980, Richard A. Neubauer, M.D, published his observations on 262 patients with MS using Hyperbaric Oxygen Therapy. His clinical impression was that "patients who received the therapy and continued with occasional follow-up treatments did not progress as far or as rapidly as those who never received the therapy." Fischer (1983) studied 40 patients with advanced chronic MS who were randomly divided into two groups and treated at 2.0 ATA for 90 minutes for twenty treatments. The experimental group received pure oxygen, and the placebo group received 10 per cent oxygen and 90 per cent nitrogen. Objective improvement (mobility, fatigue, balance and bladder function) occurred in 12 of 17 patients treated with hyperbaric oxygen and in 1 of 20 patients treated with placebo. Improvement was transient in seven and long-lasting in five. Those with less severe forms of the disease had a more favorable and lasting response. At one year of follow-up, deterioration was noticed in 2 patients (12 per cent) in the oxygen group, neither of whom had had an initial response, and in 11 patients (55 per cent) in the placebo group. Barnes (1985) used similar parameters to Fischer (90 minutes, 2.0 ATA and 20 treatments) and found improvements in bladder function in 12 of 51 patients in the hyperbaric oxygen group. The bladder improvement was present after 1 month of treatment and was maintained for 6 months without additional treatment. Oriani et al (1990) studied 44 MS patients - 22 in the 100% oxygen group and 22 in the compressed normal air group. Both receiving 2.5 ATA for 90 minutes initially for 1 month then multiple "booster" treatments over a 1 year period. In the Hyperbaric group, 14/22 reported benefits, 4 reported no change and 4 declined vs. 2 in the Hyperbaric air group reporting benefit. Pallota et al. (1986) followed 22 MS patients for 8 years. All MS patients had an initial course of 20 Hyperbaric Oxygen Treatments, and 11 were treated thereafter with two Hyperbaric treatments every 3 weeks. The frequency of relapses decreased dramatically in the long term treatment group whereas they increased in the group which received the initial treatment. |
|||||||||||||||||
|
UK DataIn the United Kingdom a charity called "The MS National Therapy Centres" installed Hyperbaric facilities across the UK. Since 1982 over 25,000 MS patients were treated with more than 3,000,000 individual Hyperbaric treatments (without a significant incident). Seven hundred and three patients were followed in detail since first receiving their treatment. The study was predominantly females (66%) with Chronic progressive MS. UK MS Therapy Centres Protocol
After twenty treatments, 70 % of patients obtained relief of two or more symptoms. In general, the response was better in patients with less advanced disease. Further assessments were made between 2 and 4 years, and again between 6 and 8 years after the initial course. They suggested that the initial improvements were being maintained by regular treatment. A third survey was conducted between 10 and 14 years, out of 446 patients, 103 (23 %) were no worse after regular treatment for 10–14 years and 30 patients (7 %) actually improved An analysis suggested that one treatment every 2 weeks was required to retard the progression of relapsing/remitting state where as once weekly was even more effective. |
|||||||||||||||||
Improvement after initial 20 treatments
Specific abilities also improved after the initial course such as Brushing teeth, doing up buttons, holding a cup, brushing hair and many of these maintained after four years. 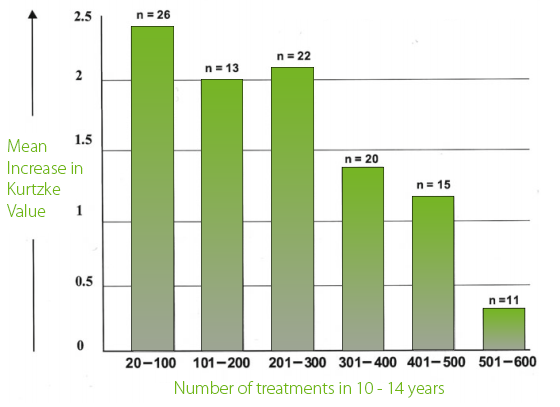 The MS patients who received HBOT most frequently over a 10-14 year period deteriorated least. The Naturopathic Approach to MS:Dr. Muradov focuses on many areas in his MS patients but there are a few key areas often considered: Gut Integrity & Dietary Augmentation, Infectious Triggers, Toxic Triggers. Diets we consider: Swank, Dairy and Gluten Free, Paleo, AIP, Low Lectin, Ketogenic, Wahls and Carnivore and idiosyncratic triggers through IgG testing. We dive deeper into gut health, with comprehensive stool cultures with PCR to identify pathogenic inflammation driving agents affecting our Edmonton patients. Infectious Triggers are screened for: Candida, Mycoplasma, Chlamydia, HHV-6 and EBV. In Dr. Muradov's experience, Viral triggers seem to dominate in young Edmonton patients with Autoimmune diseases, MS included. Screening for Lyme disease in MS patients is occasionally fruitful as misdiagnosis between the two is possible albeit rare in our experience. IV Treatment can frequently be helpful for our Edmonton MS patients. IV Glutathione is an effective option for acute inflammation. IV Therapy with B Vitamins can be helpful for energy and mood. NAD+ IV is a newer promising option for energy in MS. Ultimately, our Naturopaths will construct a unique evidence based protocol to meet the needs of your particular MS. Need help with MS?
|
|||||||||||||||||

Edmonton’s Trusted IV TherapyMultiple Sclerosis Support in EdmontonRestoring Energy, Immunity, and Neurological Function NaturallyAt TruMed Naturopathic Clinic in Edmonton, we focus on advanced natural and functional treatments to support patients living with Multiple Sclerosis (MS). MS is a chronic autoimmune condition that damages the protective myelin sheath surrounding nerve fibers, resulting in fatigue, weakness, brain fog, numbness, and mobility issues. Our MS support program integrates IV therapy, NAD+ IVs, Iron infusions, Myers Cocktails, and Hyperbaric Oxygen Therapy (HBOT)—each addressing key physiological challenges of MS such as mitochondrial dysfunction, oxidative stress, and impaired oxygen metabolism. IV Therapy for Multiple SclerosisNutrient Delivery for Energy, Immunity, and Neurological RepairPatients with MS often experience nutrient deficiencies caused by inflammation, oxidative stress, and immune dysregulation. Oral supplementation can be limited by poor absorption, whereas IV therapy delivers high doses of vitamins, minerals, and antioxidants directly into circulation. At TruMed Clinic, our IV formulations for MS are customized to provide B vitamins, magnesium, vitamin C, and glutathione—key cofactors for mitochondrial energy and myelin integrity. Benefits of IV Therapy for MS
Patients often report improvements in stamina, focus, and muscle relaxation following a series of treatments. NAD+ IV Therapy in EdmontonMitochondrial and Neurological RecoveryResearch shows that NAD+ (nicotinamide adenine dinucleotide) levels decline in neurodegenerative and autoimmune conditions, including Multiple Sclerosis. NAD+ fuels mitochondrial ATP production and regulates inflammatory gene expression—both crucial for nerve health. At TruMed Naturopathic Clinic, our NAD+ IV therapy supports brain energy metabolism and may help reduce the fatigue and cognitive slowing that many MS patients experience. Benefits of NAD+ IV Therapy for MS
Our NAD+ protocols range from 250–1000 mg per session, often combined with Vitamin Cocktails, Glutathione pushes, or Myers IVs to support the Krebs cycle and reduce oxidative stress. Iron Infusions for Multiple SclerosisSupporting Oxygenation and Red Blood Cell FunctionLow ferritin and suboptimal iron metabolism are common in chronic inflammatory conditions, including MS. Iron is essential for oxygen transport, myelin production, and brain mitochondrial activity. At TruMed, we offer medically supervised IV iron infusions to restore iron stores and optimize oxygen delivery. Benefits of IV Iron in MS
We primarily use Monoferric® (ferric derisomaltose) for one-session repletion or Venofer® (iron sucrose) for gradual correction. Myers Cocktail IVs for Multiple SclerosisReplenishing Nutrients and Reducing FatigueThe Myers Cocktail IV is one of our most popular treatments for MS-related fatigue and nutrient depletion. Benefits of the Myers Cocktail in MS
At TruMed Clinic, we typically administer weekly Myers IVs for several weeks to build nutrient reserves, followed by monthly boosters. Hyperbaric Chambers for Multiple Sclerosis in EdmontonOxygenation, Neuroprotection, and Inflammation ControlHyperbaric Oxygen Therapy (HBOT) has been studied extensively in neurological and inflammatory conditions, including Multiple Sclerosis. How HBOT Supports MS Recovery
Combining HBOT with IV TherapyAt TruMed, we often integrate HBOT with our IV programs:
Typical protocols include 2–4 HBOT sessions per week for several weeks, complemented by IV therapy for comprehensive support. Why Choose TruMed Clinic for Multiple Sclerosis Support in Edmonton
Begin Your Multiple Sclerosis Recovery Program in EdmontonIf you’re living with MS and want to explore complementary, science-based therapies for energy, cognition, and neurological resilience, TruMed Naturopathic Clinic offers advanced integrative solutions. Our IV therapy, NAD+ infusions, Iron treatments, Myers Cocktails, and Hyperbaric Oxygen sessions are designed to optimize oxygenation, support nerve repair, and restore vitality. Book your consultation today to learn how TruMed can help you enhance energy, protect your nervous system, and regain quality of life.
This section targets the unique needs of Multiple Sclerosis (MS) patients in the Edmonton area. It balances the latest 2024-2026 neuro-immunology research with a focus on symptom management and quality of life. Managing Multiple Sclerosis: The Role of Hyperbaric Oxygen Therapy in EdmontonMultiple Sclerosis (MS) is a complex challenge, often characterized by unpredictable flare-ups, chronic fatigue, and mobility hurdles. At our Hyperbaric Clinic in Edmonton, we utilize Hyperbaric Oxygen Therapy (HBOT) as a supportive, adjunctive treatment to help manage these symptoms and improve daily vitality. By increasing the oxygen levels in your blood plasma and cerebrospinal fluid, we aim to support the body’s natural neuroprotective and anti-inflammatory mechanisms. The Science: How a Hyperbaric Chamber Supports MS RecoveryResearch into MS often focuses on "hypoxia-like" environments within the central nervous system where inflammation has restricted blood flow. Using a hyperbaric chamber in Edmonton can help address these areas through several evidence-based pathways:
Real-World Benefits for Edmonton PatientsWhen searching for hyperbaric oxygen therapy Edmonton, many patients look for improvements in their "invisible" symptoms. Clinical observations and long-term reviews suggest that consistent HBOT can impact:
Your Specialized MS Protocol in EdmontonAt our Edmonton Hyperbaric Clinic, we understand that MS requires a long-term strategy rather than a "quick fix."
Research References
|